

The Missing Layer in Organisational Change
Why Change Projects Keeps Prescribing Without Diagnosing

Hi there, I’m Robert. I write about behavior change in organizations.
For more: aimforbehavior | Training | SHIFT Method
I’ve spent the last decade working inside organisations that are trying to change how people work…from tech rollouts, restructures, culture programs and process overhauls. It’s funny to think that while the contexts are always different, the pattern is somewhat the same.
These changes usually start when leadership signs off on the change, then a project team makes a plan, things start happening, the comms go out… and three months after all the excitement (or not) the change that the org was working towards is a bit stuck and nobody can formally explain why.
If you ask the change/transformation team, they will tell you did everything the methodology told them to do… which makes it even more frustrating for them, because they followed the playbook and it didn’t quite work.
My goal has been to understand why this is, and after reviewing many toolkits for change and being in the trenches… the answer is almost always the same: nobody diagnosed why people weren’t changing their behavior in the first place… they went straight from ‘people aren’t doing the thing’ to ‘let’s communicate harder’.
I decided to write this piece to highlight that missing step, so that teams and organization working on change can not only be aware of it, but can do something about it. Specifically, I want to show you where the gap is, what it’s costing, and introduce a methodology I’ve built called SHIFT that’s designed to close it. In a follow-up article I’ll walk you through the full process step by step.
The premise problem
The dominant practice in change management tends to default to a familiar cluster: vision, messaging, stakeholder engagement, and resistance management…even when the real barriers may sit in the workflow, systems, or norms.
This has been evident and as I mentioned earlier when looking at frameworks spanning public sector, corporate, international development, professional certification, and academia. The toolkits differ in “packaging” sure, however they converge on the same premise… communicate the change well enough, align enough people, build enough readiness, and the behavior will follow.
That premise isn’t wrong… but it’s incomplete for how change happens in work as done scenarios… the ones we all experience basically.
The contact centre that trained people who already knew the process
A government contact centre was rolling out a new compliance system, and for some reason the adoption was very low… what did we hear? That the reason people were resistant was because we needed to provide them with more training… which to me sounded a bit incomplete as a reason.
Nevertheless, the director asked for the training materials to be redesigned and for someone to run all the trainings… so… after checking and seeing the numbers quite low still, we validated that was not the issue.
Thankfully I was able to convince the director to let us do a deeper diagnosis to see what was actually happening…and low and behold… the new system required 14 clicks to log a single customer interaction… who wanted to go through 14 steps… they workaround took only 3.
It goes to show you that the people were not resisting because they didnt want the change, or because they were acting irrationally, it was the system that made the old way better than then new one.
See, no amount of training or comms was going to fix that issue..and this is why knowing the actual barriers helps you focus on the right solution.. in this case it was redesigning the workflow interface.
This kind of misdiagnosis happens constantly.. because the dominant frameworks for change don’t have a diagnostic layer. they have a communication layer, a readiness layer, a stakeholder management layer… and assume the diagnosis has already happened.
What diagnosis actually means in a change context
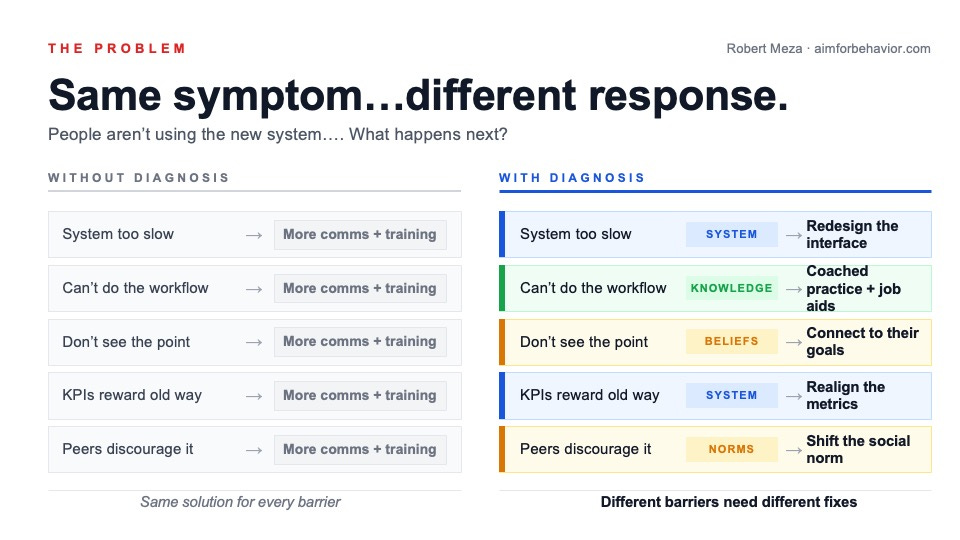
In medicine, you don’t prescribe treatment before identifying the condition, because the same symptom can point to dozens of different causes, each needing a different approach.
Organisational change should work the same way…the symptom is almost always identical, people aren’t doing the new thing… but the root cause varies enormously, and the right approach depends entirely on which root cause you’re dealing with.
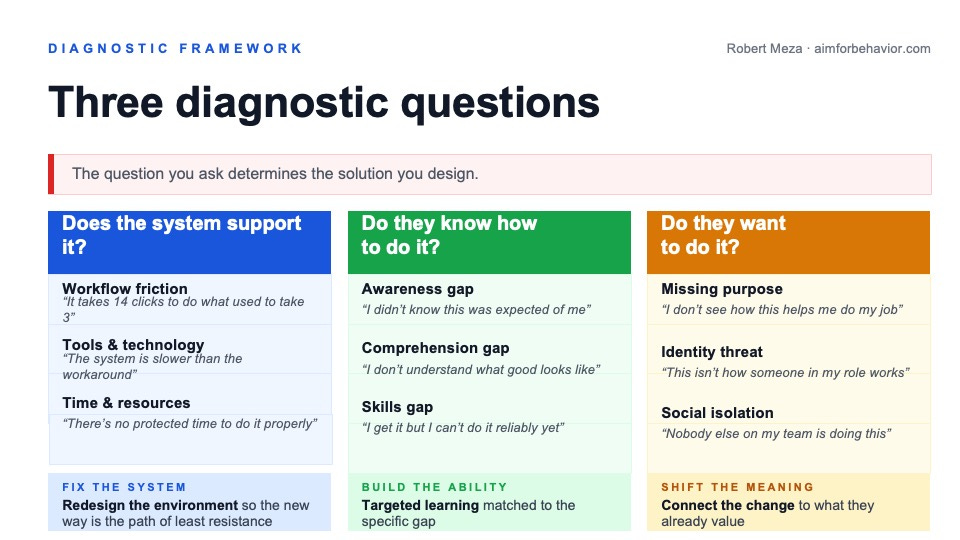
Behavioral science gives us three diagnostic questions here…. they draw on well-established research into what drives and blocks human behavior, particularly the work of Susan Michie and colleagues at UCL. The core insight is simple… every behaviour has three preconditions, and when any one is missing, the behaviour won’t happen.
Does the system support the change? Do people have the time, tools, resources, and support they need? Someone whose system takes 14 clicks when the old one took 3 doesn’t have a mindset problem. They have a system problem and the fix is redesigning the environment, not running another training session.
Do the people know how to do it? Do they have the knowledge, skills, and cognitive capacity to actually do the thing under real working conditions? Not in a training room, but at their desk, under pressure, on a Tuesday afternoon. If they can’t, that’s a knowledge and ability barrier and training might actually be the right call here.
Do they want to do it? Do they see why it matters to them personally? Does the change conflict with their identity, their beliefs, or what their peers expect? Someone who has the tools and the skills but can’t see how the change connects to anything they care about has a willingness barrier…and that needs a completely different conversation than training or comms.
Here’s the thing you need to know: the fix for each question is completely different.
-Training doesn’t fix a system problem
-Communication doesn’t fix a knowledge gap
-Incentives don’t fix broken environmental design
Many orgs aren’t able to make this distinction and end up defaulting to asking for “more training and more comms” from the change and transformation teams regardless of what’s actually blocking people.
Why the field is skipping diagnosis
It’s worth asking why the dominant methodologies skip this step.. it’s not because the people who built them are careless.. I think it is because they’re solving a different problem.
Kotter’s 8 Steps solves for leadership alignment and momentum, while ADKAR for example solves for individual readiness… and yes, each of these is useful for something, but none of them is designed to answer: what specific behavior needs to happen, what’s blocking it, and what mechanism actually addresses that block?
They work at the level of the programme, while diagnosis works at the level of the behavior…those are very different altitudes.
Now, I know what some of you are thinking… well ADKAR does separate Knowledge from Ability. That’s fair, however, there’s a real difference between putting a label on a gap and diagnosing its mechanism. When ADKAR says there’s a “Desire” gap, it gives you engagement tactics, but It doesn’t tell you whether that gap is missing purpose, identity threat, or social isolation. And those are very different problems that need very different fixes. “Desire is low” is a label, not a diagnosis. A label tells you where the problem is, but a diagnosis tells you what to do about it.
The field has a diagnostic gap. Existing frameworks are strong at mobilising a programme, but they’re weaker at diagnosing behavior-level barriers and matching them to interventions. That’s not a criticism, it’s an observation about where the next layer of value sits.
SHIFT: a different premise for change
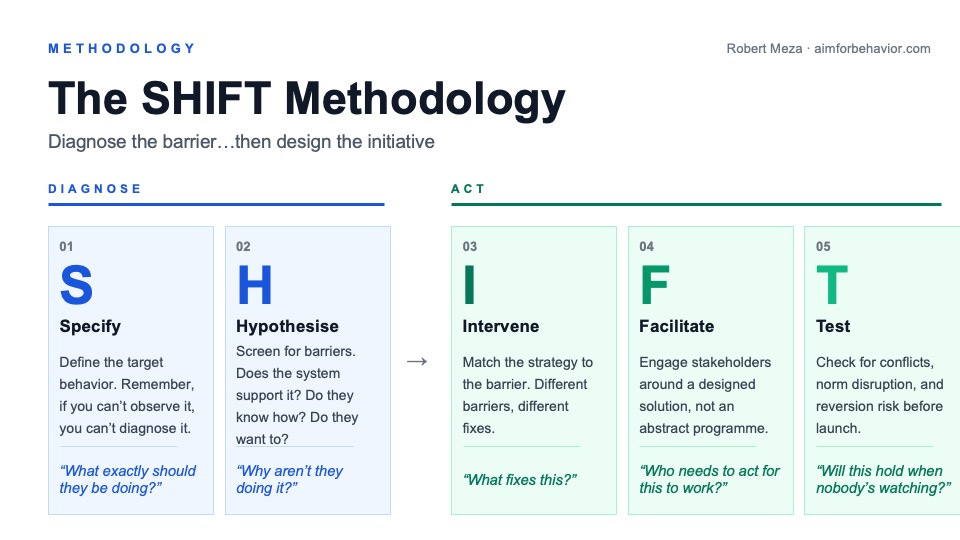
SHIFT stands for Specify, Hypothesise, Intervene, Facilitate, Test. It’s my behavioral/implementation science methodology for organisational change that starts from a different place than the traditional ones it asks:
What specific behaviors need to happen?
What’s preventing them?
What mechanism addresses that barrier?
In what sequence should we apply the interventions?
That’s a fundamentally different starting point.. which is more about engineering a system of interventions matched to specific barriers.
Really, this is why I made SHIFT in the first place and why I have been training teams on it and brining into consulting work.
I didn’t make SHIFT to replace what you’re already using, instead it sits underneath your existing methodology, not in competition with it. When Kotter’s coalition is built but adoption isnt there, SHIFT diagnoses why. When ADKAR identifies a gap, SHIFT unpacks what kind of gap it is and routes it to a matched intervention… as people who have been using it in their companies have told me, It’s the diagnostic layer that the other frameworks assume has already been done.
Here’s what each phase does…I’ll walk through the full process with worked examples in the next post.
Specify the target behavior using our ABC Tool (Actor/Behavior/Context) We make sure we go away from “improve safety culture”, which is vague, to something you can actually see and diagnose…Most change programs go light on this step or may skip it, which is not a good place to start your program.
Hypothesise the barriers by asking the three diagnostic questions. Does the system support it? Do they know how to do it? Do they want to do it? But go deeper than just the three questions. Within the wanting to question alone, “low buy-in” could mean missing purpose, identity threat, or social isolation… and each one needs a different fix. Another thing practitioners may miss: barriers travel in clusters…a skills deficit almost always shows up alongside a confidence gap, which means If you only address one, the other keeps the behavior from moving.
Intervene with strategies matched to the specific barrier you’ve found. If they don’t know how, structured learning. If the system doesn’t support it, redesign the defaults. If they don’t see why it matters, connect the change to something they already care about — not the org’s vision deck. Sequencing matters too: build the ability before you try to shift the meaning, fix the system before you try to change attitudes. I keep seeing this — what looks like a willingness problem just disappears once you remove the structural barrier. People who seemed “resistant” were making a rational choice given a badly designed system.
Facilitate stakeholder engagement when you have a diagnosed barrier and a matched strategy, the conversation with stakeholders becomes concrete: “Here’s what we found, here’s what we’re proposing, here’s why.,” that’s a much easier conversation than “we need your support for the change programme.”
Test, Sustain, Adapt for sustainability before you go live and after you have launched, because if you can’t picture the behavior sustaining in six months when nobody’s watching, your plan has a gap.
Objections I hear about diagnosing…
“This is too slow, and we need to move fast.”
Diagnosis doesn’t slow you down.. what does is misdiagnosis. a team that spends two weeks diagnosing the barrier and then deploys a matched intervention will outperform a team that skips it and spends six months iterating on the wrong one.
“We already know what the problem is.”
Maybe you do know the problem…but why is it that teams are running their program for months without the results they expected, if you already knew the problem, the interventions would be working.
“Our people just don’t like change.”
This is the one I hear most, and it’s almost never accurate… people change all the time, they change jobs, move cities, learn new tech and so on. They do new behaviors when those behaviors solve a problem they actually care about…. what people don’t like is being asked to do something harder than the current way, with no clear personal benefit, while the people asking them to change haven’t changed anything about their own behavior. We can’t keep calling this resistance, because what it is, is a rational response to a poorly designed system.
“We’re already using proven change models, so why do we need this?”
You don’t need to replace what you’re using., but you do need the layer that’s missing underneath it, the diagnostic one that is so often underused.
Five things you can do this week
You don’t need to use my full methodology… but you should use it to help you think critically and build your mental model of diagnosis.
Write your behavioral statement. Pick the single most important behavior your change program requires and write it as Actor-Behavior-Context. If you can’t make it observable, keep refining until you can. Make sure you spend the time here as everything downstream depends on it.
Run the 3-question diagnostic. For that behavior: Does the system support it? Do they know how to do it? Do they want to do it? Write down your insights for each.
Check your strategy-barrier match. Look at whatever interventions/initiatives you’ve already got planned, and for each one, ask: which specific barrier does this address? If the answer is “all of them” or “general resistance” you will have a match problem, because an intervention that addresses everything addresses nothing.
Talk to five people who aren’t changing. Not their managers, not the project team, but the actual people whose behavior needs to change. I used to go up and down in my office to talk to people and understand why the CRM wasn’t being used… this is where they showed me the excel that was being used as a workaround and told me why. I listen for the difference between I don’t know how (knowledge gap), the system makes it difficult (system barrier), and I don’t see why this matters (belief barrier). These conversations will tell you things the dashboards can’t
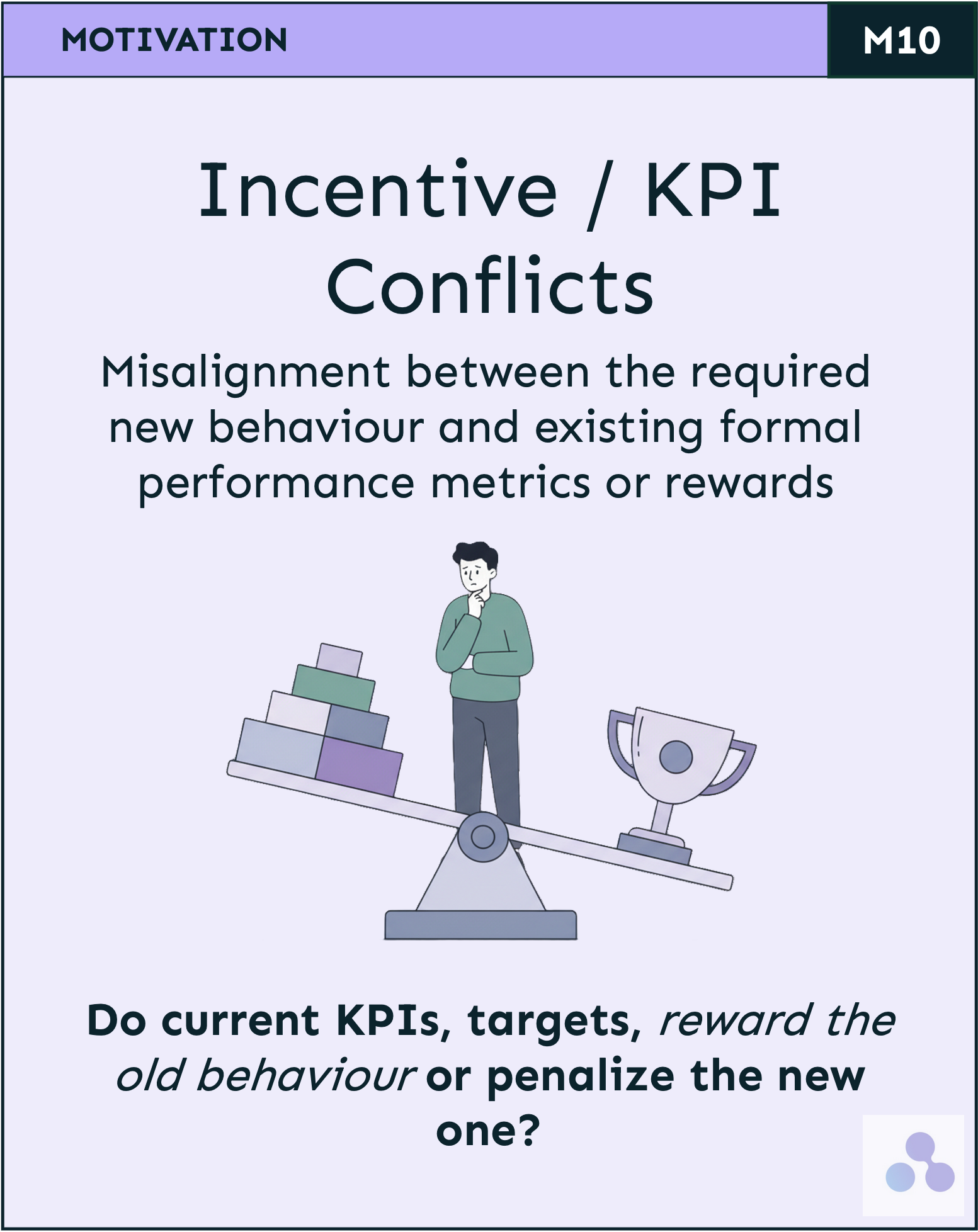
Test one intervention for conflict. Pick your most important planned initiative and ask: does this contradict anything else we’re doing? If you’re asking people to take ownership while mandating exactly how they do it, you have a conflict. These contradictions are invisible from the project plan and obvious from the front line.
What comes next
The organizational change field isn’t broken… It’s just incomplete as it is being practiced.
The communication and stakeholder work that existing methodologies provide is genuinely useful, its the map, but it is not always going to work as the navigation system, because it’s not diagnostic.
SHIFT adds that diagnostic layer underneath, and you can start using the thinking behind it this week. Write the ABC, ask the three questions, sit down with the people who aren’t changing…the answers are usually right there, waiting for someone to ask.
In a future post: I’ll walk through each phase of SHIFT in detail, including a full CRM scenario from a project I worked on.
I write about behavioural science for organisational change every week...subscribe to get the next one.
And if you’re working on a change program where the behaviour isn’t changing, I’d be curious to hear what you’re seeing… reply to this email or find me on LinkedIn.
Have a great day,
Robert
Brilliant insight about the diagnosis gap. This resonates deeply with something I just explored: we're training people to communicate with machines with surgical precision while leaders still struggle to brief their own teams clearly. The missing layer you describe—understanding why behavior needs to change—connects directly to communication clarity. If leaders can't articulate the 'why' and expectations, change stalls. https://creatism.substack.com/p/we-prompt-machines-better-than-we?r=177ve
I wish people would test! I wish I wish I wish!